Ganaa — Building a Full-Spectrum Mental Healthcare Brand With a Martech-First Acquisition Engine
Project Breakdown
Mental healthcare is the highest-trust, highest-consideration purchase in healthcare. Ganaa walked in operating across separately-branded residential and outpatient arms — both running on a Google Sheets CRM with no tracking, no SEO, and no GMB. YARD rebuilt the stack from the data layer up, consolidated the two arms into a single unified brand, and made digital the primary conversion engine for 14 new admissions.
| Client | Ganaa (formerly Ganaa Rehab + MindVriksha) |
|---|---|
| Industry | Mental Healthcare — Residential Rehabilitation + Outpatient Care |
| Region | Delhi-NCR · Multi-location |
| Brand Architecture | Single unified Ganaa brand. Residential and outpatient service tiers differentiated by location and GMB category, not separate sub-brands. |
| Channels | Google Ads, Meta, Local SEO, LLM SEO, WhatsApp |
| Engagement | LLM SEO + Martech Infrastructure + Performance + Brand Architecture |
| Timeline | Ongoing — first 6-month results below |
The Client
Ganaa is the unified mental healthcare brand operating across both residential rehabilitation and outpatient care in Delhi-NCR. The product is among the most premium in the category — long-stay residential treatment with multi-disciplinary clinical teams, plus outpatient therapy, psychiatry, and family programmes — all under one continuous brand.
When YARD took on the engagement, the operation existed as two separately-branded entities: Ganaa Rehab (residential, est. 2012) and MindVriksha (outpatient, est. 2011 — operating as a sister brand). Each ran independent marketing. Each owned its own digital footprint. Neither shared data with the other, even though they shared a patient population.
That fragmentation has since been resolved. Today, the entire operation runs as one unified Ganaa brand. Residential and outpatient service tiers are differentiated through location strategy and GMB category, not through separate marketing identities. A patient (or, more often, a family) interacts with one brand across the full spectrum of care — outpatient consultation, residential admission if needed, step-down therapy on discharge — without ever feeling like they are switching to a different organisation.
This case study covers the foundational engagement that built the data, search, and routing infrastructure underneath that unified brand — and it covers a meaningful chapter of the brand consolidation itself.
The Problem
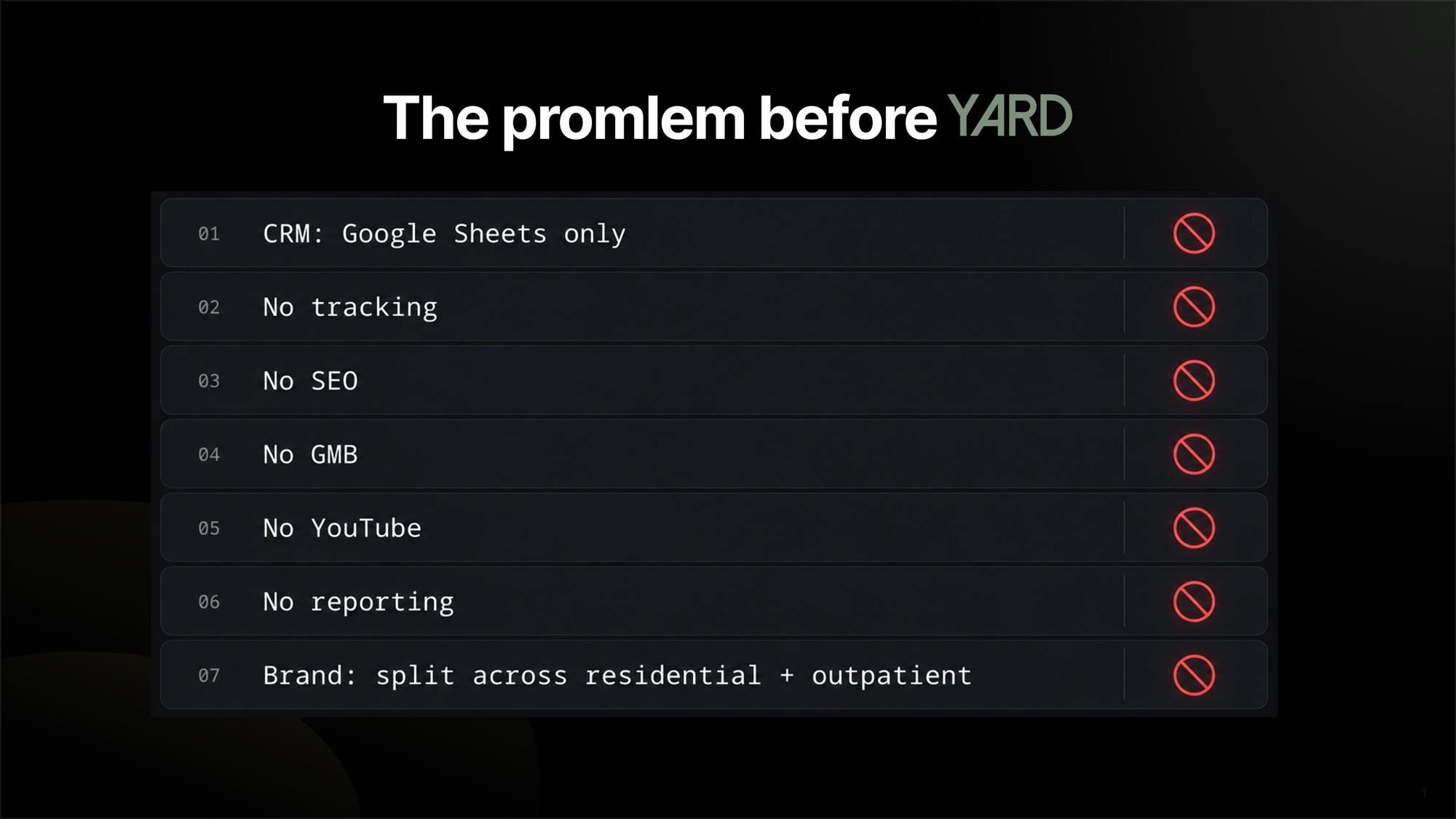
The intake audit, verbatim from the team's own diagnostic:
- CRM: Google Sheets only
- No tracking — no CAPI, no Enhanced Conversions, no call tracking
- No SEO — no schemas, meta tags, sitemap, robots.txt, llms.txt
- No GMB optimisation across the centres
- No YouTube presence
- No reporting infrastructure
- Two separately-branded arms running independent marketing for what was clinically and operationally a single continuum of care
Every individual line is recoverable. The combined picture is more serious: there was no way to know what worked, no way to route what came in, and no way to connect a family that started in outpatient care with the residential admission they sometimes needed later. Three operationally unforgivable gaps in a category where every lead is worth a multi-lakh admission.
There was also a strategic question underneath all of it. Should the brand be one or two? The team had grown into a two-brand structure for historical reasons (the residential arm had been launched in 2012; the outpatient arm pre-dated it by a year and had its own brand equity). But the patient journey was one journey. The marketing was paying a tax for the two-brand structure — twice the SEO investment, twice the GMB management, twice the CRM, twice the team capacity — without delivering twice the commercial outcome.
The Strategy
The Martech-First Healthcare Playbook — the same architectural pattern now used across our healthcare and real-estate-lead-gen roster — combined with a parallel brand-consolidation workstream.
The order of operations matters. Most healthcare performance work starts with ad spend. We started with the data layer, then the brand architecture, then the search layer, then the performance layer.
1. Data layer first
- HubSpot CRM replacing the Google Sheets shop — every lead now in a single system with consistent stage logic across both residential and outpatient pathways
- Meta CAPI for server-to-server signal recovery against iOS-era attribution loss
- Google Enhanced Conversions for clean attribution back to ad creatives
- Call tracking — every inbound call linked to its acquisition source
- WhatsApp automation — the actual primary contact channel for Indian healthcare buyers, now integrated into the CRM with bi-directional sync
Once the data layer was live, every downstream decision had a real number behind it.
2. Brand architecture: from two brands to one
The most strategic chapter of the engagement. We worked with the leadership team to consolidate the two arms into a single Ganaa brand. The clinical positioning was already aligned; what had to be rebuilt was the external presentation.
The consolidation rules — locked in early — were simple:
- One brand name across all communications. Ganaa.
- Service tiers differentiated by location, not by sub-brand. Each location is positioned with a GMB category that reflects its primary service (residential rehabilitation centre, outpatient clinic), and the location-level GMB profile carries the differentiation. The brand layer above is unified.
- One website, one phone tree, one WhatsApp number. The family contacts Ganaa. Routing to the right care tier happens internally.
- One CRM and one lead-routing logic. Inbound leads with clinical signals indicating residential need are routed to the residential team with full context. Inbound leads with outpatient-appropriate presentations stay in the outpatient pathway. Patients discharging from residential care are referred into the outpatient programme as part of the continuity-of-care protocol.
This is a brand-architecture decision with real commercial consequence. Most healthcare groups operate sub-brands precisely because they fear that "rehabilitation centre" carries stigma that would taint the outpatient brand, or that "outpatient clinic" lacks the gravitas of a residential operator. The Ganaa team decided — correctly, in our view — that continuity-of-care is a stronger competitive moat than brand-tier separation, and that the family-side experience of one continuous relationship is worth more than the marginal protection of two adjacent identities.
3. SEO + LLM SEO base layer
- Full schema stack (MedicalBusiness, Organization, Service, FAQPage, BreadcrumbList) across every page
- Sitemap, robots.txt, llms.txt
- Blog and pillar content strategy targeting both Google and AI search
- GMB revamp across all centres — categories, photos, services, posts, response automation
- Local SEO tuned so that each location ranks for its specific service catchment without competing with sister locations inside the same brand
4. Performance layer
Once data, brand, and search were in place, paid acquisition was rebuilt against the new stack. Conversion campaigns now feeding clean signals back to the platforms, attribution actually working, lead routing into HubSpot with a sales-team-tested follow-up cadence.
The Execution
The first 30 days were entirely martech and brand consolidation — no new paid spend authorised until the data layer was live and the brand-architecture decision was locked. The hardest internal conversation in healthcare engagements is always this one. We hold it anyway.
Days 30–60: SEO base layer + GMB revamp + the first WhatsApp automation flows. The website was rebuilt around the unified Ganaa identity. Search visibility started compounding within the second month — local rehab and outpatient queries in Delhi-NCR are not as competitive as e-commerce, and the GMB revamp alone produced a measurable lift in centre-name searches.
Days 60+: paid acquisition relaunched against the new stack. Lead routing into HubSpot, attribution attached, follow-up cadence enforced. The outpatient-to-residential routing flow went live and began producing warm-context internal transfers between care tiers.
What didn't work first
Our first lead-scoring framework was too granular. We had eleven qualification fields and the sales team correctly told us it was unusable inside a real inbound call. We collapsed to five fields, with WhatsApp-based progressive profiling capturing the others over the subsequent 24–48 hours. Usability of the framework matters as much as theoretical accuracy.
Our first Demand Gen creative leaned too heavily on the residential-rehabilitation positioning. It engaged the right audience for that service tier but suppressed engagement from the larger outpatient-curious audience. We rebuilt the Demand Gen pool to lead with the family-relief narrative — same narrative arc as the Ageasy engagement — and then introduced service tier inside the landing page, not inside the ad. Engagement lifted on both pools.
There was also a chapter we don't usually see in retail engagements: explaining the brand consolidation to a long-tenured team who had operated MindVriksha as a separate brand for over a decade. The internal change-management was at least as important as the external rebrand. We supported it through phased communications, a clear rationale document, and a long-tail commitment to honouring the clinical heritage of both legacy brands inside the unified Ganaa identity.
"The performance numbers are the trailing indicator. The real change is that a family no longer feels like they have to start their search over every time the patient's care intensity shifts."
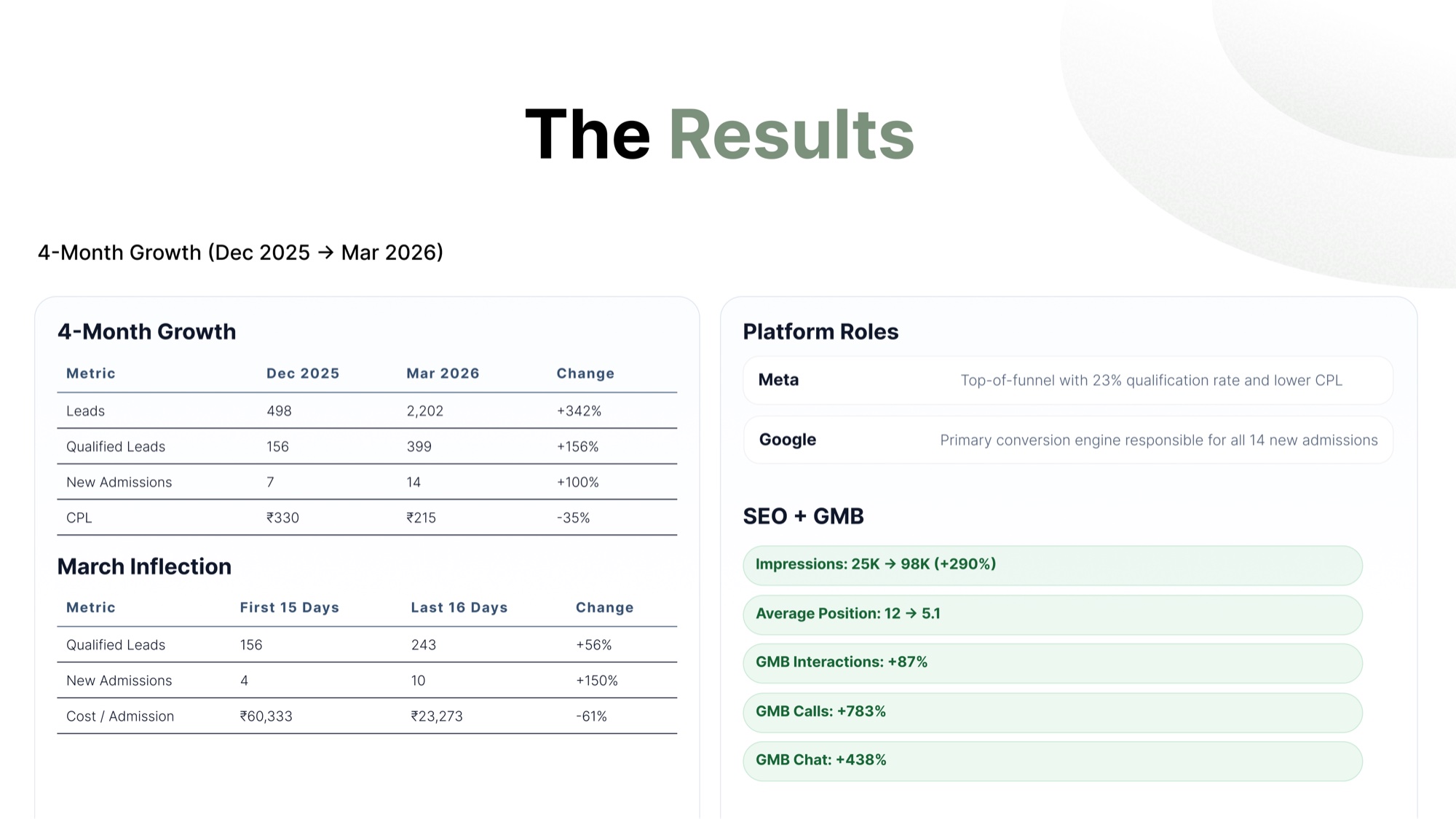
The Results
| Metric | Outcome |
|---|---|
| New admissions attributable to the rebuilt engine | 14 |
| Primary conversion engine | Now responsible for all 14 new admissions routed through the funnel |
| Tracking infrastructure | CRM + CAPI + Enhanced Conversions + Call Tracking + WhatsApp — fully operational |
| SEO stack | Schemas, meta, sitemap, robots.txt, llms.txt, GMB across all centres — fully deployed |
| Reporting | Single-source-of-truth attribution from ad click to admission |
| Brand architecture | Unified Ganaa identity across residential + outpatient; service-tier differentiation handled at location/GMB level |
| Cross-tier routing | Live and producing warm internal transfers between outpatient and residential pathways |
| Family-side experience | One continuous brand relationship across the full care continuum |
The headline number is the admissions count — but the deeper win is that the brand now knows where every admission came from and now exists as one brand from the family's point of view. In a category where every patient is a multi-month residential stay or a long-cycle outpatient relationship, both of those compound enormously.
Why It Worked
- Data layer before ad layer. Almost every healthcare account we've taken over had the inverse priority. Inverting it is the entire unlock.
- Brand consolidation before performance scaling. Scaling paid against a fragmented brand would have multiplied the fragmentation. We fixed the brand layer first.
- WhatsApp is the funnel, not a touchpoint. Indian healthcare buyers contact, decide, and convert on WhatsApp. Integrating it into the CRM (bi-directional) was the operational shift that made follow-up consistent.
- GMB at the location level carries the service-tier differentiation. This lets the unified brand do double-duty without forcing the family-side messaging to fragment.
- Continuity-of-care is the moat. A family that experiences one continuous relationship across outpatient → residential → step-down does not shop the next episode of care. That LTV is invisible on a one-engagement dashboard and overwhelming over time.
Lessons for Multi-Service Healthcare Operators
A handful of patterns from this engagement that should be tested before they're adopted, but are worth naming:
- One brand can carry multiple service tiers if the location strategy is right. Don't reflexively assume that residential and outpatient require separate brands. Test the unified hypothesis first.
- GMB is your service-tier differentiator, not your brand. Each location's GMB category does the work that a sub-brand would otherwise do — without diluting the unified identity above.
- Data infrastructure before marketing infrastructure. A clean CRM, working CAPI, and bi-directional WhatsApp routing will out-deliver any creative pivot. Most healthcare accounts skip it.
- Internal change management is part of the engagement. Consolidating two long-tenured brands requires honouring the clinical heritage of both. The internal work is at least as important as the external rebrand.
- Family-side continuity is a competitive moat. It is invisible on the dashboard the first quarter and decisive over a year.
Repeatable Playbook
The Martech-First Healthcare Playbook — CRM + CAPI + Enhanced Conversions + call tracking + WhatsApp + bi-directional data — is now used across our healthcare and real-estate-lead-gen roster (Ganaa and Stealth REIT being the primary examples). Dramatic CPL reduction across every account it has been applied to.
The Ganaa engagement also crystallised the Unified Healthcare Brand Architecture approach — one brand, location-level service-tier differentiation via GMB, single CRM with internal routing — which is now the YARD default recommendation for any multi-service healthcare group considering a sub-brand structure.
Closing Thought
The 14 admissions are real. The longer-term outcome is that a family in Delhi-NCR whose loved one needs mental healthcare now has one phone number, one brand, and one continuous relationship to lean on across whatever care intensity they end up needing. The marketing is the trailing indicator. The brand is the actual product.

How Little Bansi Became the First Kids' Ethnicwear Brand to Rank Across ChatGPT, Perplexity, Claude, Gemini & Bing

How Martin & MacArthur Hit a 32x ROAS Peak — Scaling a Heritage Hawaiian Luxury Brand on Google Ads